
Photo from 2011 Naama team
Published May 24, 2012, last updated on April 7, 2020 under Voices of DGHI
Genny Olson and I will be shipping off to Mityana, Uganda in just under a week. Thanks to Dr. Ariely and Dr. Kigongo's assiduous advising, I've gone from lost and confused in November to prepared and ready to hit the ground running today (hopefully...).
Here's some background information on the community and our project goals:
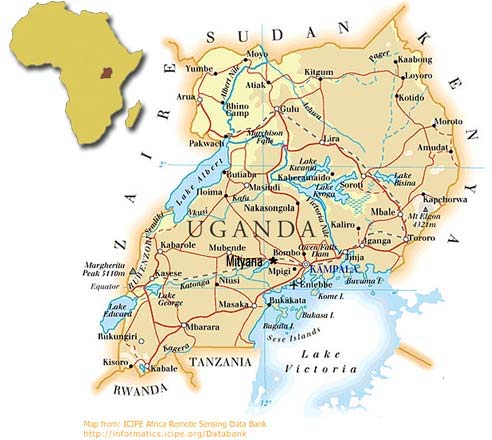
Description of Context & Community Naama is a parish (and village) in the Mityana District in Central Uganda. As of 2010, the Mityana District had an estimated population of 354,000. There are a number of villages inside of the Naama parish. Naama has complex historical roots and a variety of cultural, religious, ethnic, linguistic, and socio-economic factors that shape daily life. [1]
Naama is a relatively resource-poor community. Community members have routinely identified a lack of income generation opportunities as a key issue. Fishing and other subsistence level activities form the most common professions. However, there is a variety of wealth in the community. Some homes are reported to have running water, electricity, and refrigerators, while others are destitute, lacking in basic commodities. Diarrhea and malaria are the most prevalent health challenges in the community.
Healthcare is free and provided by the government, yet clinics are scarce, expensive, and understaffed. There is a government clinic in Naama, but the nearest hospital is in Mityana. Patients are asked to pay for the medical supplies they need and bring them to the hospital. Community members have also identified the community-based orphan problem as one of the more serious issues in the community [2].
The orphan problem in Naama, like in much of sub-Saharan Africa is extreme due to the effects of HIV/AIDS. Roughly 14% of children in Uganda are orphans (Atwine, Cantor-Graae, and Banjunirwe 555–564). The children are oftentimes “adopted” by extended family members. These children can be seeing as having lesser status and receive fewer benefits with regards to things like nutrition and education as a part of their extended family. In resource-tight situations, an extra child can place an onerous financial burden on a family. Community-based orphans have been found to be lacking in almost every measure of emotional, educational, physical, and health outcome compared to their non-orphan peers (Atwine, Cantor-Graae, and Banjunirwe 555–564).
In Naama there are Christians, Born-Again Christians, Muslims, and non-denominational individuals. The country as a whole is 85% Christian, 12% Muslim, and 2% other ("Uganda: International Religious Freedom Report 2009"). A majority of the Muslim populations live in the North. Tensions between Muslims and Christians (or North and South) have been at the source of many of Uganda’s civil issues. Museveni and the National Resistance Movement has had continuous success since 1986 because it is very inclusive and even courted many in Amin's tribe. Religion has affected the success of the counseling program because some families of community-based orphans have refused to send their children to the VOSA orphanage that hosts the counseling program, and is backed by Christians, for fear of the child being “brainwashed.” Secularizing the program could make it more accessible to the broader community. When we were sorting through the donated books for the library Genny and I debated whether or not to include the religious books. I did not want to include them to keep the program secular, but Genny insisted that those books would be the most sought after because of many children’s intense faith.
I need to work to find the balance between my Liberal, Western obsession with political correctedness and accepting certain things as inevitable, fundamental parts of the local culture. There are more than 100 NGOs in Mityana. Many of them are reportedly addressing the same issues. This speaks to the importance of collaboration and synchronicity with local efforts. The government of Uganda is structured hierarchically. The base unit is the village, identified as Local Council 1 (LC1). A number of LC1s make up the jurisdiction of a LC2 in an area known as a parish. LC3s oversee a number of parishes in an area known as a sub-county. This structure continues to the county and district level with LC4s and LC5s. Each official is responsible for public health efforts in his/her jurisdiction to varying degrees.
People in Naama speak Lugandan and English, as well as a variety of other languages spoken within the region. English skills are generally associated with education, and the most impoverished and rural individuals are least likely to speak English. This will be a big challenge for Genny and I as together we will be conducting close to 200 interviews with our partner and translator, Robinah.
Our Aims and Goals Genny and I will be working in Naama on a variety of projects as a part of the Naama Community Health Collaboration, a program that has been in operation since the summer of 2008. Our main project is a household-mapping project. The purpose of this project is to develop a tool that local government officials can use to build a database of public health indicators. We just need to figure out the best information to collect. Which questions succinctly reap useful data? Are there questions people do not answer? We will create a sample instrument and then use it on a 100 random households in randomly selected villages within the Mityana Parish, surveying 10 households per village. (View our current template here. Feedback is appreciated!)
The goal is to empower Local Council 1 and Local Council 2 officials to manage their affairs. If children are dying from something in this area, why are they dying? Are they close to water and more exposed to malaria? Are there bad crops there and malnutrition? Understanding where and what the problems are will give the Local Council 1s the ability to efficiently respond to issues even under the financial constraints. But, public health is a small part of the governmental duties they carry out and Dr. Kigongo has had a difficult time convincing the local council officials to do the project. Officials see the logic of it, but have hesitated to do it as Dr. Kigongo has advised, pointing to opportunity costs and the lack of funds available to do projects like this. However, very recently, they have said that they will dedicate the personnel and funds to the project. Dr. Kigongo is buying a computer to enter the data in that the local officials will use.
Additionally, we will take part in the planning and execution of an annual health fair. It is a two-day event that over 1000 people attend annually. The NGOs that attend offer a number of services including testing for HIV, malaria, diabetes, and syphilis. Health professionals also offer seminars on topics such as water sanitation, malaria, family planning, and antenatal care at the event. Our role lies in organization. We will be contacting the applicable parties requesting their attendance, securing a location, holding meetings with relevant stakeholders, inviting schools to attend, inviting a guest of honor, and securing funds.
My principal individual project is a research project on the effectiveness of group counseling for improving community-based orphans emotional outcomes. I aim to offer follow-up health and emotional assessments to 35 children whose emotional and physical health was measured last year in a study conducted by Grace Zhou, who was also a duke student. By following up on Grace’s analysis and extending it, increasing the sample size, we hope to judge how access to mental health services affects the well being of community-based orphans. To provide a control, I will offer the same emotional assessments to 20 random community-based orphans who have not been attending the counseling sessions.
To gain information on the program from varied perspectives, I will also conduct focus group sessions with local primary school teachers (certified as counselors and not certified), local community leaders, and relevant stakeholders in the project in order to understand how these parties view the counseling program and the community-based orphan problem in Naama. Genny, Robinah, and I will also assist in a number of small projects, including holding an educational soccer tournament, teaching in Naama Millennium Preparatory, and assisting with the creation of a small library. Genny's Mom managed to transport 250 pounds of books to Kampala in April, and Robinah is currently cataloging them for the library! Thanks to the Blue Thong Club, TCMS, Pat Moxley, and many other donors for their generous support! We also managed to (ostensibly) increase the benefits of our travel by stuffing our bags with 150 pounds of medical supplies for a clinic in Naama (and maybe Mityana Hospital) thanks to John Lohnes and Duke Remedy - an absolutely fantastic program that "recover(s) usable surplus medical supplies and distribute them via Duke-affiliated projects to areas of need overseas." For those of you who made it this far.. first off WOW. I even skimmed it and I wrote it! Second, I promise this will be the longest blog I ever write. To end this tome, here is a beautiful quote:
"This is the true joy in life, being used for a purpose recognized by yourself as a mighty one. Being a force of nature instead of a feverish, selfish little clod of ailments and grievances, complaining that the world will not devote itself to making you happy. I am of the opinion that my life belongs to the whole community and as long as I live, it is my privilege to do for it what I can. I want to be thoroughly used up when I die, for the harder I work, the more I live. I rejoice in life for its own sake. Life is no brief candle to me. It is a sort of splendid torch which I have got hold of for the moment and I want to make it burn as brightly as possible before handing it on to future generations."
George Bernard Shaw
Until Later! CMOX
Related News

Research News
Study Highlights the Challenges of Integrating Opioid Treatment into HIV Care
December 10, 2024


{kind=link}